
Rosanna Fulchiero
Diuretic Exposure in Critically Ill Pediatric Patients Who Progress to Continuous Renal Replacement Therapy
Presenter
Rosanna is a second year pediatric nephrology fellow at the Children's Hospital of Philadelphia and a first year Masters of Science in Clinical Epidemiology student at the University of Pennsylvania. Her research interests are in the management of fluid overload in critically ill children with acute kidney injury and the pharmacoepidemiology of diuretic use in these patients.
Abstract
Background:
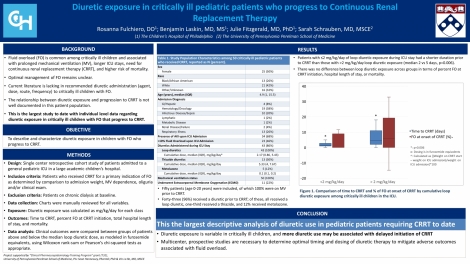
Fluid overload (FO) is common in critically ill children and associated with substantial morbidity, including prolonged mechanical ventilation (MV), longer hospital stays, need for continuous renal replacement therapy (CRRT), and higher risk of mortality. The optimal management of FO remains unclear. Current literature on recommended diuretic administration to critically ill children with FO and the relationship between diuretic exposure and progression to CRRT is lacking. In this study, we aim to describe and characterize diuretic exposure in children with FO who progressed to CRRT.
Design/Methods:
This is a single center retrospective cohort study of pediatric patients admitted to a general pediatric intensive care unit (ICU) in a large academic children’s hospital who progressed to CRRT for a primary indication of FO as determined by comparison to admission weight, MV dependence, oliguria and/or clinical exam. Charts were manually reviewed for all study variables (sex, age, admission diagnosis, presence of any acute kidney injury (defined as at least KDIGO Stage 1), MV status, percent FO at ICU admission). Diuretic exposure during ICU admission was calculated as mg/kg/day for each medication class. Outcomes included time to CRRT, percent FO at CRRT initiation, total hospital length of stay, and mortality. Clinical outcomes were compared between groups of patients above and below the median loop diuretic dose, as modeled in furosemide equivalents, using Wilcoxon rank-sum or Pearson’s chi-squared tests as appropriate.
Results:
Fifty patients (age 0-20 years) were included, of which 100% were on MV prior to CRRT. Forty-three (96%) received a diuretic prior to CRRT; of these, all received a loop diuretic, one-third received a thiazide, and 12% received metolazone. Patients with <2 mg/kg/day of loop diuretic exposure during ICU stay had significantly fewer days to initiation of CRRT than those with >2 mg/kg/day loop diuretic exposure (median 2 vs 5 days, p=0.006). There was no difference between loop diuretic exposure groups for percent FO at CRRT initiation, hospital length of stay, or mortality.
Conclusions:
To our knowledge, this is the first pediatric study to report ICU diuretic exposure in critically ill pediatric patients with FO that progressed to CRRT. Diuretic exposure is variable in critically ill children, and more research needs to be conducted to further characterize the relationship of diuretic exposure with important clinical outcomes. Multicenter, prospective studies are imperative to determine optimal timing and dosing of diuretic therapy to mitigate adverse outcomes associated with fluid overload.
Keywords
acute kidney injury, renal replacement therapy, fluid overload, pediatric, diureticsAbout Us
To understand health and disease today, we need new thinking and novel science —the kind we create when multiple disciplines work together from the ground up. That is why this department has put forward a bold vision in population-health science: a single academic home for biostatistics, epidemiology and informatics.
© 2023 Trustees of the University of Pennsylvania. All rights reserved.. | Disclaimer